TAVI is a means of replacing an aortic valve in the heart through a catheter-based approach and may be used as a less invasive alternative to surgical aortic valve replacement (AVR), which is a major operation involving open-heart surgery and requiring a reasonable level of fitness from the patient in order to be successful.
TAVI was selected for the study because NHS standards, published in 2013, suggest that only experienced surgeons should be carrying out these procedures. The standards also suggest that provider volume is an important factor in TAVI outcomes, believing that ‘occasional practice and small volume TAVI units should be actively discouraged’ and TAVI programmes should aim to carry out at least 50 procedures per year.
TAVI is a relatively new intervention and in 2013 there was a limited evidence base around procedural outcomes. Dr Foster’s investigation aimed to explore the effects of surgeon and provider annual volume on TAVI mortality rates and whether a correlation between these could be established.
Dr Foster’s analysis of TAVI procedures was undertaken alongside an analysis of conventional elective AVR for comparison. Using data from Hospital Episode Statistics, the study analysed 43,089 elective AVR and 13,887 elective TAVI procedures between April 2010 and March 2019, considering first operations only. The mortality indicator included deaths 30 days post-op, and annual volume included any AVR or TAVI procedure performed by the provider and surgeon within the year prior to the index procedure.
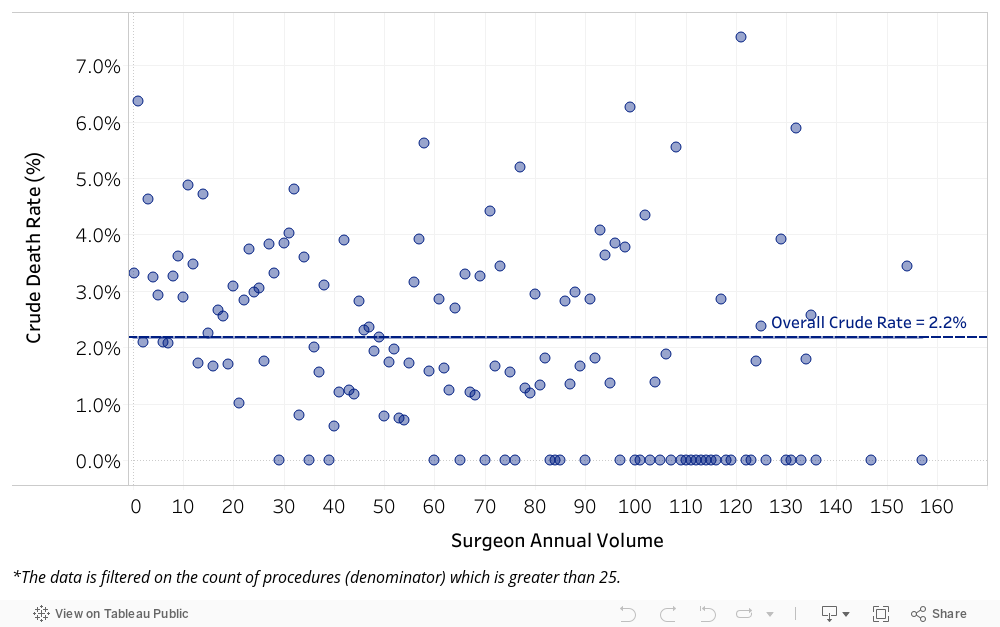
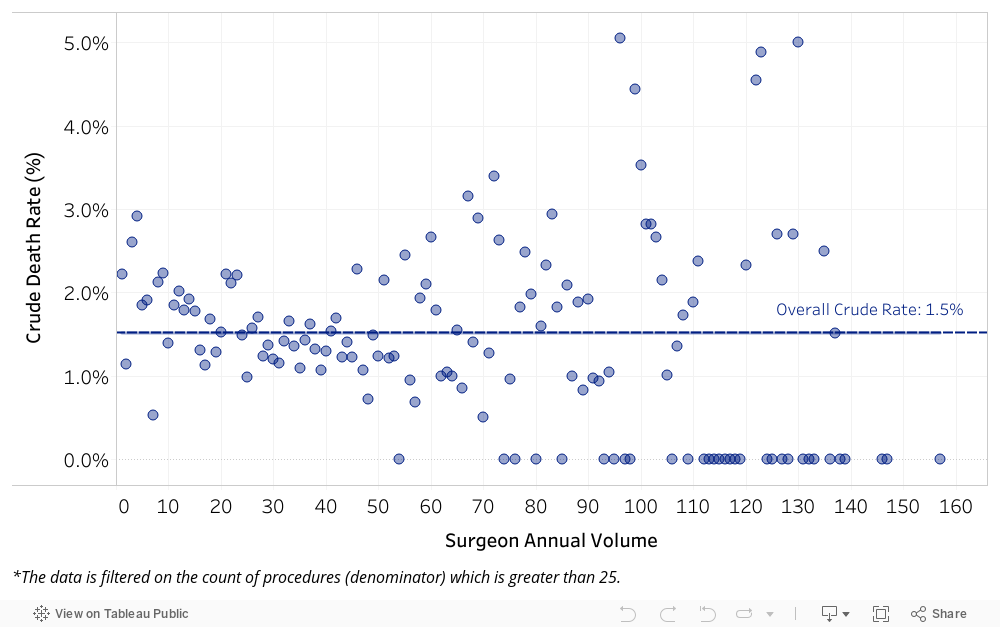
Overall crude mortality rates for TAVI and AVR were 2.2% and 1.5% respectively (Figures 1 and 4).
Multi-level logistic regression models, including surgeon and provider level random effects and adjusting for case-mix (age, gender, deprivation, calendar year, comorbidities), were used to understand the effect of surgeon and provider annual volume on mortality outcomes. Interestingly, the results differed for both procedures.
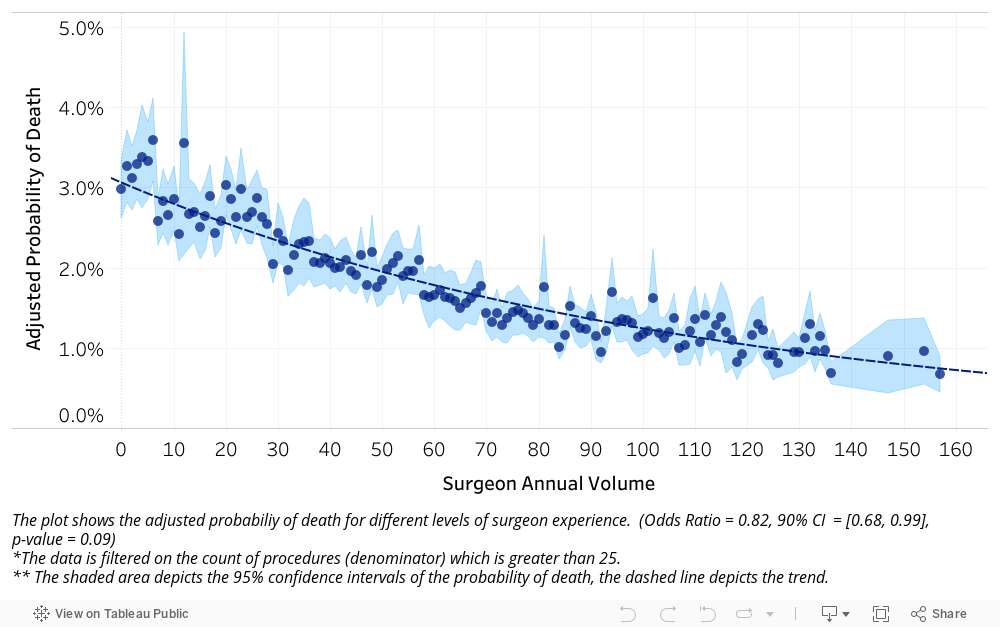
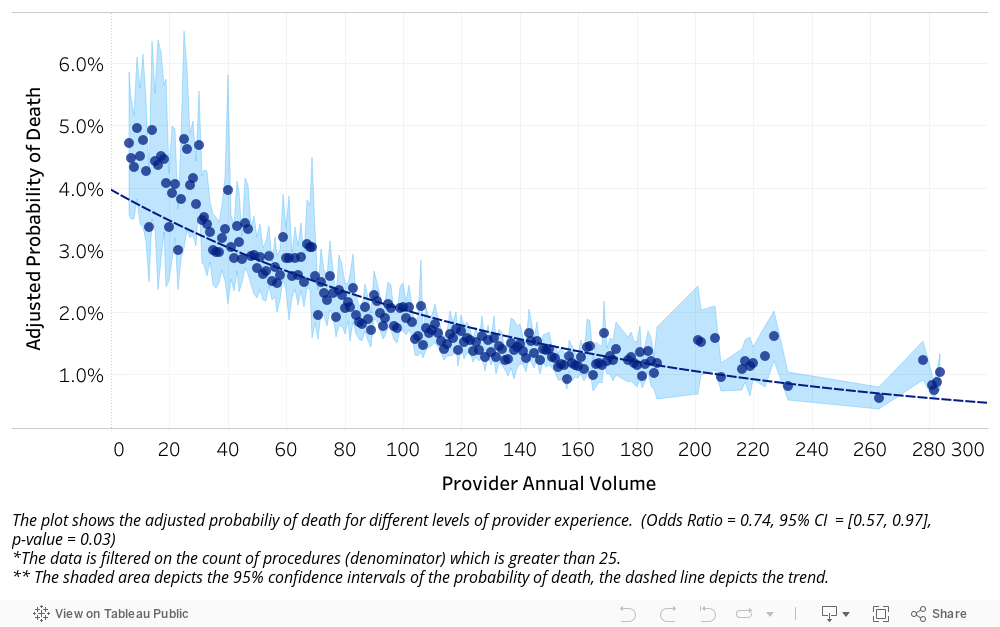
For TAVI surgeries, surgeon experience showed a negative correlation with adjusted mortality, which suggests that more experience does equate to better outcomes. This was, however, found to be only a marginally significant factor (Figure 2). Provider volume was found to be more significant (p-value = 0.03), showing an exponential decrease in the adjusted mortality rate as provider volume increased (Figure 3).
Figure 1 – Crude mortality rate by level of surgeon experience for TAVI
Figure 2 – Adjusted risk of death by level of surgeon experience for TAVI
Figure 3 – Adjusted risk of death by level of provider experience for TAVI
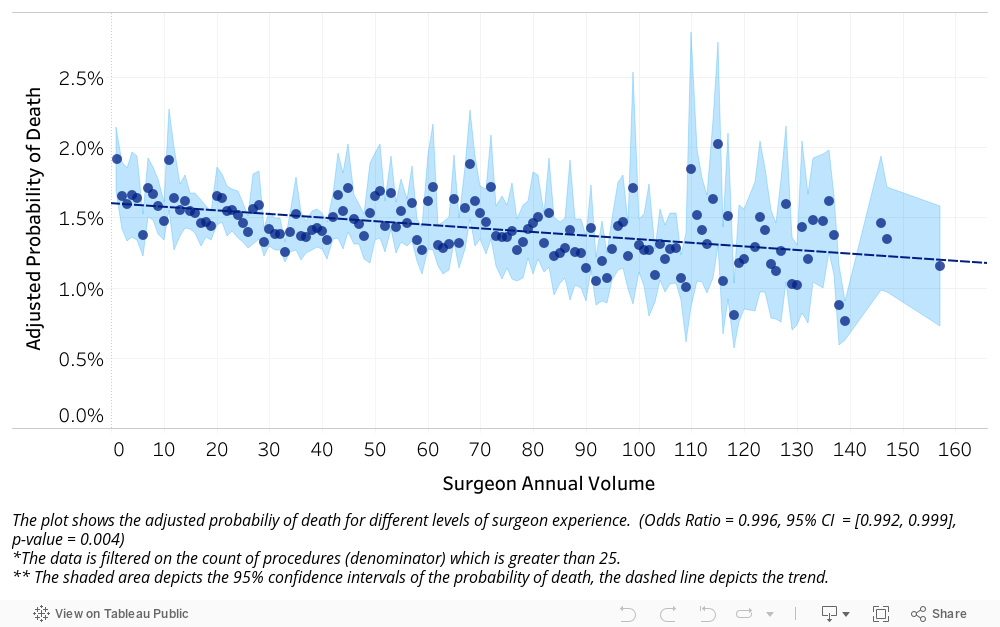
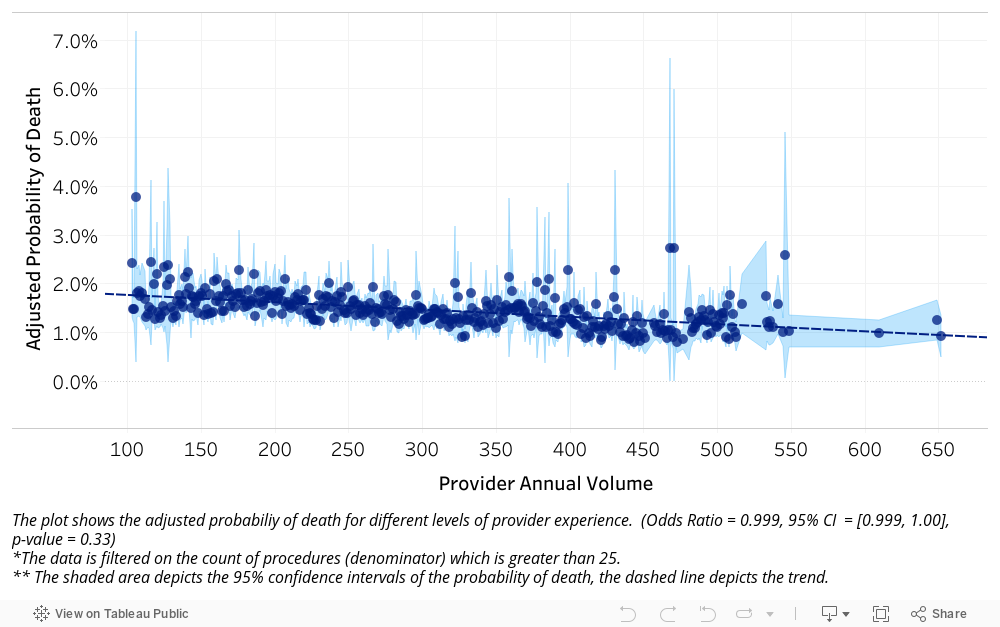
Conversely, for AVR procedures surgeon experience was highly significant (p = 0.004) and showed a gradual decrease in mortality as surgeon experience increased (Figure 5). Provider volume, however, was not significant and showed little correlation with mortality (Figure 6).
Figure 4 – Crude mortality rate by level of surgeon experience for AVR
Figure 5 – Adjusted risk of death by level of surgeon experience for AVR
Figure 6 – Adjusted risk of death by level of provider experience for AVR
This kind of study is crucial in giving patients an informed choice about where they have their procedure, or who performs it. A patient considering where to have a TAVI surgery performed would want a hospital that performs a high volume of these surgeries overall, whereas an AVR patient would instead look at surgeon-level volume.
The results of the analyses are also relevant to service redesign in the NHS. The decrease in TAVI mortality rates with higher provider volume supports the view that hospitals should become more specialised in their procedural offering rather than having the same services replicated at every acute setting. This would mean higher volumes of surgeries, such as TAVI, for specific hospitals, which would deliver better outcomes for patients. Greater integration across systems would therefore be beneficial, and influential factors such as provider volume should be closely examined and considered when services are being commissioned.
For more information on Dr Foster’s analytical capabilities contact us here