
Quantifying NHS activity reduction during the peak of the COVID-19 crisis
14 Oct 2020
14 Oct 2020
There has been widespread concern around the potential longer-term public health impact of the pandemic and, as NHS trusts work to restore elective services, Dr Foster has undertaken an in-depth analysis of activity reduction using Hospital Episode Statistics to help paint a clearer picture of how spell volume and diagnosis rates were affected during the peak of the crisis.
The analysis found that, across the board, there was a significant reduction in elective spell volume during April-May 2020, with some diagnosis groups showing a staggering 90 per cent drop. Cancer diagnoses rates fell. There was also a marked reduction in emergency activity, with the exception of childbirth and, unsurprisingly, viral infections, which showed a huge increase of 242 per cent across both months.
Interestingly, the analysis also found that fewer patients presented with cardiac dysrhythmias, which may be the result of people avoiding healthcare facilities for risk of overburdening services or becoming infected with COVID-19. This is of particular concern as missed diagnoses of these types of conditions can increase the risk of complications further down the line.
At trust level, the study showed a large volume drop in both elective and non-elective activity across all organisations. Overall, the analysis suggests that the long-term effects of the pandemic are likely to be far-reaching, with a future spike in demand possible due to missed diagnoses and postponed procedures. Cancers may now require a greater level of treatment, or even be untreatable, if they have been left undetected or untreated as a result of the crisis. Further analysis at trust-level is needed to help organisations understand their backlog and which services and patients to prioritise.
During the peak of the pandemic in the UK, the NHS cancelled elective activity in order to ensure all available resources were focused on the influx of potentially acutely ill coronavirus patients and prevent the system from becoming overwhelmed. As a result, in April we noticed an activity reduction for the majority of the most common diagnosis and procedure groups. In order to quantify this reduction, we have used data from the Hospital Episode Statistics (HES) database to compare the observed spell volume for diagnosis/procedure groups in April 2020 with their expected volume. This is based off a five-year trend line for the same month, in order to account for seasonal variability and population growth.
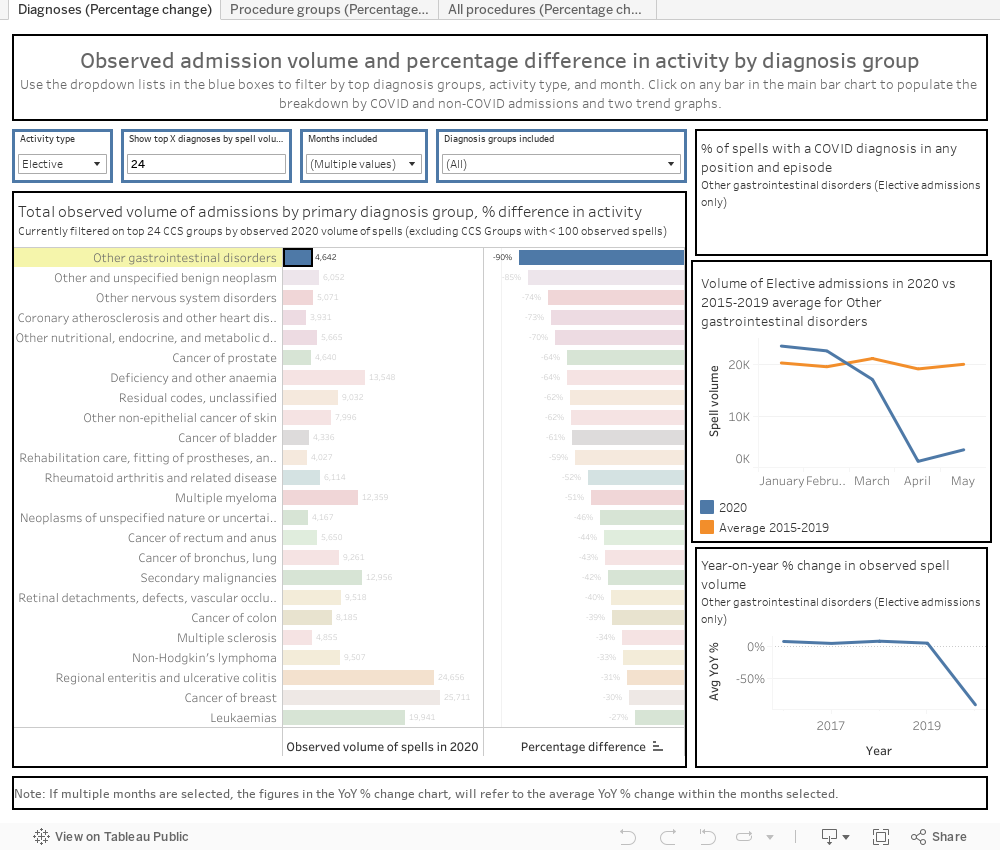
Where appropriate, this analysis will also look at the year-on-year percentage change in observed activity, in order to determine if differences between observed and expected volumes are likely due to the pandemic or are in line with normal variability. When using the dashboard, we suggest focusing on diagnosis groups with high volumes of observed activity, rather than smaller volumes with perhaps a large percentage reduction in activity, as these instances will likely be more subject to natural variation. The supplementary graphs that appear when selecting a particular diagnosis or procedure group provide more in-depth information on historic trends in activity.
Elective spell volume for all diagnosis groups, with only a few exceptions, was found to be lower in April/May 2020 than expected, with some diagnosis groups showing a 90 per cent reduction in observed admissions compared with the expected rate. Such drop-offs in activity could be attributed to the pandemic as shown by the differences in observed volume in 2020 compared with the average for 2015-2019.
In particular, elective cancer diagnoses fell below expected levels as well as year-on-year (compared with April and May 2019). Breast cancer diagnoses fell 30 per cent below expected, colon cancer 39 per cent, prostate cancer 64 per cent, and cervical cancer 32 per cent.
Non-elective diagnoses also fell below expected volumes. Septicaemia, COPD, and skin/subcutaneous tissue infections fell 65 per cent, 57 per cent and 52 per cent below expected levels respectively. The only non-elective diagnosis, aside from childbirth and conditions associated with labour, to see an increase in activity was viral infections, which shot up to 421 per cent above the expected volume in April, and fell to 86% above expected volume in May. In 79 per cent of these spells, the patient tested positive for COVID-19. Interestingly, as pneumonia cases fell by 49 per cent, it could be the case that some patients may have been diagnosed with COVID-19 as an incidental finding while also being treated for pneumonia. Childbirth was 4 per cent above the expected level and could be seen as a control diagnosis showing normal levels of variability, as this is one diagnosis group we can assume was unaffected by the pandemic.
It is concerning to see that fewer people are presenting with cardiac dysrhythmias, as the longer these go untreated, the greater the risk of complications. For example, if atrial fibrillation goes untreated, it places patients at risk of transient ischaemic attacks and strokes. Arrhythmias can also cause heart failure if not adequately managed. Across April and May, 3,662 fewer patients than expected nationally, based on the projection from the last five years of data, had acute myocardial assigned to their admission as the primary diagnosis, and 5,668 fewer patients (a 38 per cent reduction) had non-hypertensive congestive cardiac failure as their primary diagnosis. This could imply missed diagnosis, leading to delayed treatment of conditions that require timely management to prevent disease progression.
In addition, there was a 41 per cent reduction in the number of patients presenting with nonspecific cardiac chest pain and a 44 per cent reduction in those with abdominal pain. This means that fewer patients with very common vague signs and symptoms were presenting to hospital in the first instance, reducing the potential for follow-up appointments and investigations that may lead to definitive diagnoses. In April and May, patients with common respiratory conditions, such as acute bronchitis, COPD, and bronchiectasis, as the primary diagnosis showed a 68 per cent and 57 per cent respective reduction in volume of admissions. These large decreases could indicate that patients with pre-existing respiratory conditions were more perturbed by an admission to hospital than perhaps other patients were and sought options to manage their conditions in the community.
Outside of delivery, elective procedures fell in 2020, with some volumes reduced to 98 per cent below expected levels.
Cancer-related elective procedures also saw drop-offs in activity, as expected. Chemotherapy and radiotherapy observed volumes were found to be 32 per cent and 49 per cent below their expected volumes respectively.
Non-elective chemotherapy and radiology observed procedures also saw drops down to 41 per cent and 33 per cent below expected levels respectively.
The reduction in elective upper and lower GI tract endoscopic procedures is stark (91-92 per cent in both). These include predominantly colonoscopies and gastroscopies, both of which are key in the investigation and diagnosis of cancers of the GI tract. Additionally, emergency diagnostic imaging (with the exception of heart) showed a 24 per cent reduction, which equates to 42,693 fewer admissions. This could delay the diagnosis of a range of health conditions normally identified with imaging techniques such as CT and MRI scans.
So far, the percentage changes and volumes of patients have looked at the primary diagnosis in the admission, which is taken from a single episode in the spell. However, the all-procedures dashboard looks across the entire spell in all episodes, for specific diagnostic cardiology and common procedures, allowing Dr Foster to identify a greater volume of admissions where the procedure was performed.
Elective cardiology procedures fell greatly against expected levels for April and May 2020. Percutaneous transluminal ablations of heart fell to 84 per cent below expected levels, with similar drops seen for coronary artery bypass graft (CABG) (75 per cent), coronary angiograms (76 per cent), valve surgeries (62 per cent), PCIs (percutaneous coronary intervention: 62 per cent) and insertion of pacemakers/defibrillators (55 per cent).
Non-elective cardiology procedures saw similar declines in volume. CABG (70 per cent), coronary angiograms (45 per cent), valve surgeries (48 per cent), insertion of pacemakers/defibrillators (39 per cent) and PCIs (23 per cent) all saw drops below their expected levels.
Overall elective and non-elective spell volume for trusts fell across the country, with no trust recording above their expected volume in April. Observed non-elective spell volume was 12 per cent to 50 per cent lower than expected across all trusts, and elective spell volume was 48 per cent to 91 per cent lower than expected.
The fall in volume of activity seen in April and May 2020 represents a major concern for patients. Large reductions in activity related to signs, symptoms, and diagnostic checks will mean more serious conditions may go undiagnosed. Cancer Research UK claims that over 24,000 cases of cancer have gone undiagnosed during the pandemic, with some becoming inoperable.
In order to determine the impact of this activity reduction on mortality, two possible follow-up analyses could be done into the mortality rates of acute coronary syndrome (ACS) and cancer patients both during and after April/May 2020. The first would look at the effect of missed early diagnoses and cancelled diagnostic procedures on mortality rates, while the second would investigate the effect of cancelled operations involving patients already diagnosed with cancers/ACS on mortality. Both analyses would have to include deaths in all settings and people who died of complications related to ACS/cancer.
The challenge for hospital managers now is to figure out the best way to prioritise patients with non-COVID-19 diagnoses. It may also be necessary to encourage patients to willingly attend hospitals for signs and symptoms who have been otherwise avoiding hospital for fear of catching COVID-19 or “unnecessarily” using overstretched NHS resources. Activity reduction analyses could be run on trust-level HES data or local data, which would be more up to date than HES data. Such analyses could enable trusts to gain an in-depth understanding of their current backload and potentially help decide which patients are most in need of reopened care services.
Get the latest insights and updates from Telstra Health UK.
View now

