Analysis reveals correlation between surgeon annual volume and mortality for the repair of abdominal aortic aneurysms
04 Sep 2019
04 Sep 2019
An AAA repair is typically performed on patients that have an enlarged aorta exceeding 5.5cm and there are two procedures available. One option is an open procedure, which involves a large incision made in the abdomen of a patient to insert a graft. The other is an endovascular (EVAR) procedure, which involves making a small incision in the groin through which instruments are inserted into the artery via a catheter and threaded up to the aneurysm. A stent and graft are then placed to support the aneurysm.
Using Hospital Episode Statistics data, we analysed 11,745 elective open AAA repairs and 24,544 elective EVAR AAA repairs between April 2009 and March 2019. Surgeon annual volume included any repair of AAA performed by the surgeon within the year prior to the index procedure. The study adjusted for case-mix (age on admission, sex, index of multiple deprivation, and comorbidities that tested significant including congestive heart failure and renal disease) as well as provider annual volume and year of index operation.
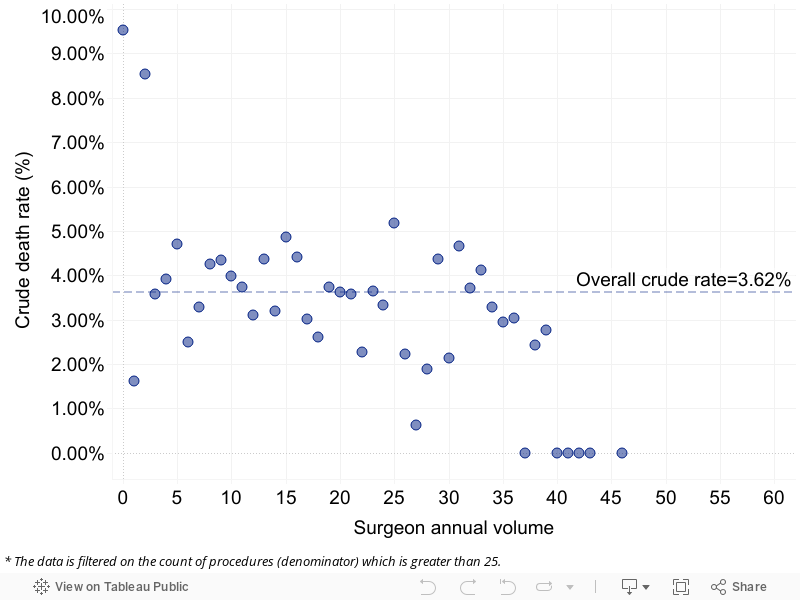
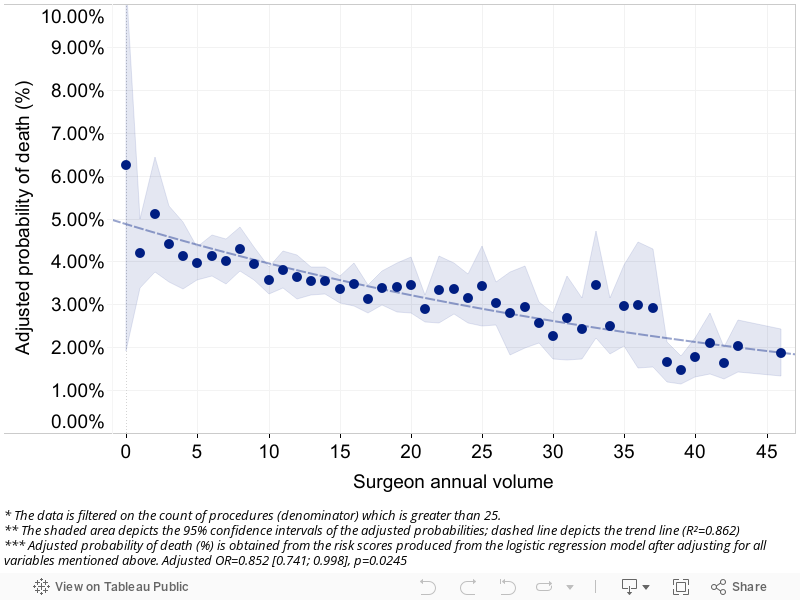
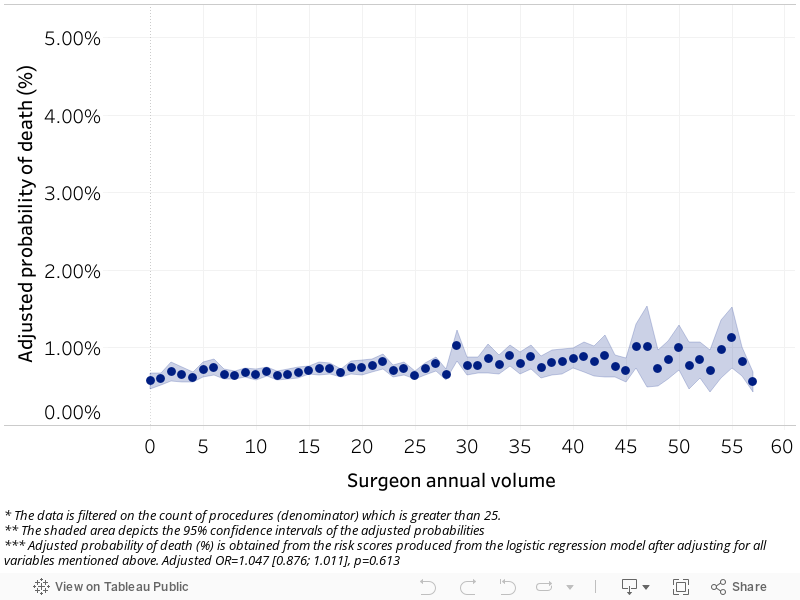
For open repairs of AAA, surgeon annual volume was found to be a significant variable influencing mortality, with a strong negative exponential trend (Figure 2). It was not found to be statistically significant for mortality following EVAR procedures (Figure 4). Respectively, the crude rates of mortality were 3.62 per cent and 0.75 per cent as shown in Figures 1 and 3. The analysis suggests that an increase in the number of AAA repairs a surgeon performs in a year would marginally decrease the odds of mortality following open procedures.
Our Consultant Focus tool provides an overview of consultant-level activity covering admitted and outpatient volumes, case-mix, and outcomes, within an organisation or at a national level. A consultant’s performance can be analysed over a specific time period up to five years and is then benchmarked against the consultant’s specialty. This provides a comprehensive picture of a consultant’s practice, including scale and quality, and enables trusts to work closely with consultants to improve mortality.
Dr Foster has significant statistical expertise in surgical performance combined with expertise in outcomes frameworks, national clinical improvement programmes and bespoke analytics. Our analysts work with NHS trusts to define the indicators, determine the baseline for each indicator and then calculate a target to achieve through interventions. All indicators are verified by the Dr Foster Unit at Imperial College to ensure they are statistically robust. This means that all outcomes are measured in a meaningful way and allow for comparisons over time and between different entities.
Indicators are adjusted for demographics and other factors such as comorbidities, and consultants use statistical techniques to ascertain whether differences are statistically significant or the result of chance. This is important to ensure changes are not made in response to random fluctuations.

Get the latest insights and updates from Telstra Health UK.
View now

